



Story highlights
Chris Lihosit?was saved by umbilical cord blood?from three babies used to treat Leukemia
Cord blood banking is still the exception rather than the norm
In early August 2015, Chris Lihosit fell ill with an exhausting, dehydrating and pyjama-soaking fever that mysteriously disappeared two days later.
During a check-up, on his 43rd birthday, his doctor named summertime flu the most likely culprit.
Then the same thing happened again, and it settled into a disturbing pattern: midweek chills and an escalating fever that would break on Sunday. By Monday, Chris would feel fine, only to have the sequence repeat itself.
He joked about it with colleagues at T-Mobile, where he works in software development, “Well, I hope it’s not cancer!”
On alternating weekends from May to October, Chris would volunteer as a back country ranger for the US Forest Service – a physically demanding role that involves patrolling Washington’s Cascade Mountain forests and hiking along high-altitude trails with a backpack that can weigh up to 32 kilograms.
But now, even at sea level, he was getting winded just walking his two dogs around the block. What was going on?

A medical appointment revealed a heart murmur and suspicions of endocarditis, an infection of the heart’s inner lining. The scare triggered another series of tests that led Chris and his husband, Bill Sechter, to Emergency Room 4 at the University of Washington Medical Center.
A whiteboard checklist documented his Saturday morning: insertion of a large-bore IV as a potential conduit for antibiotics, a round of blood draws, and discussions with the ER doctor.
Then the phone rang and the nurse answered, listened and responded to multiple questions in quick succession: “Yes. Yes. Oh, OK. OK. Yeah.” He excused himself from the room and soon returned in a “full hazmat suit”, as Chris describes it. Yellow.
“And that’s when we were like, ‘Oh s***, it’s on. Something is seriously bad.’”
Chris learned that his level of infection-fighting neutrophil cells, normally churned out by the bone marrow, had fallen so low that his defenses were in tatters. He was also severely anemic, with roughly half the normal amount of red blood cells in his blood.
It wasn’t endocarditis. And when one of his doctors performed a blood smear, she saw something on the microscope slide that shouldn’t be there: blasts.
These leukemic cells, stuck in adolescence, were the harbingers of the coming horde that had so astonished 19th-century surgeons.
The doctor apologetically broke the news and Chris and his sister dissolved into tears. In an emotional Facebook post later that day, he attached a picture of himself in a hospital gown and pink face mask and wrote: “this avowed agnostic could actually go for your good juju / positive thoughts or even your (gasp) prayers.”
More tests, including a bone marrow biopsy of his pelvic bone, painted an increasingly disturbing picture. He had acute myeloid leukaemia, a fast-progressing cancer.
The biopsy suggested that an astonishing 80 per cent of his bone marrow cells were cancerous. Strike one.

Other results suggested that chemotherapy wouldn’t be as effective on his form of leukemia. Strike two.
And genetic tests put him in the unfavorable risk category by revealing that his cancer cells carried only one copy of chromosome 21, a rare anomaly associated with “dismal” outcomes, according to recent studies. Strike three.
Chris needed to start chemotherapy immediately.
But first, he had his sperm banked. Then, with family and a close friend at his side, he celebrated his impending treatment with prime rib and cheap champagne smuggled into his hospital room.
Over three days, he received multiple doses of the anticancer drugs cladribine, cytarabine and mitoxantrone, the last a dark blue concoction often dubbed “Blue Thunder.” The drug turned his urine a shade he describes as “Seahawks green” in honor of Seattle’s football team. Other patients have had the whites of their eyes temporarily turn blue.
On the third night of his drug infusion, a sudden back pain grew into an intense pressure in his chest that felt like he was being stabbed. A heart attack? An emergency CAT scan instead revealed two newly formed blood clots: one in his right leg and another in his right lung – not uncommon consequences of chemotherapy.
Over the next six months, Chris would need transfusions of blood-clotting platelets whenever his level of them dipped too low, and daily injections of a blood-thinning drug whenever it rose too high.
Thirteen days after being admitted into the hospital, he posted a more hopeful Facebook entry: “And I’m finally going home! Now the real adventure begins.”
New hope
Based on his leukemia classification, Chris was braced for multiple rounds of chemotherapy. He and his husband were overjoyed when a second bone marrow biopsy suggested that the leukemia had become undetectable after only a single round.
Because of his high-risk classification, however, Chris’s doctors said that the cancer was likely to return without a bone marrow transplant.

But Chris discovered that he had inherited an extremely rare set of cell-identifying protein tags. Only one bone marrow donor on the worldwide registry matched his genetic tags, and that person was unable to donate.
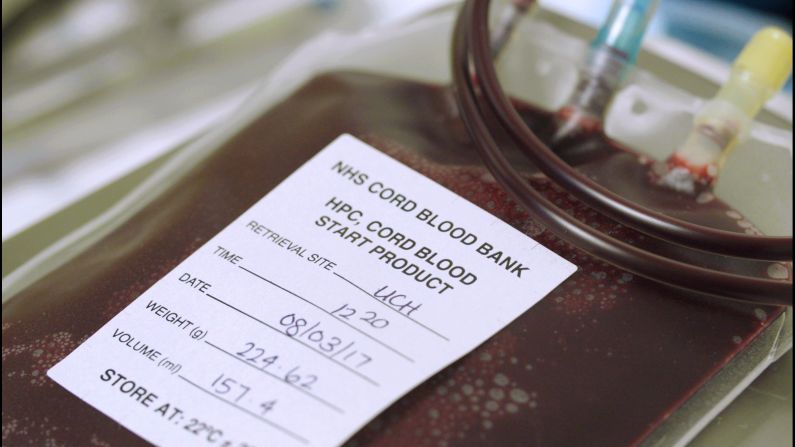
An umbilical cord blood transplant, Chris and his doctors agreed, was his best hope.
Like bone marrow, cord blood is unusually rich in hematopoietic stem cells – which can give rise to every type of blood cell – and their more developed descendants, progenitor cells, which are more limited in what they can become. But, unlike bone marrow, cord blood can be collected in advance and stored for decades in liquid nitrogen.
First, Chris would need to spend another five days in the hospital for a standard follow-up round of chemotherapy to pick off any hidden cancer cells. Chris marked the occasion with a Facebook post of himself in a grey felt Viking helmet and attached braids. “Round 2… And FIGHT!” This time, the chemo went off without a hitch.
He was a familiar face at the medical center, though, with three additional hospitalizations: twice for bacteremia, a bacterial blood infection marked by high fevers, and once so doctors could tame an allergic reaction to a transfusion of platelets, which always reminded Chris of chicken broth.

He had to steel himself again on Christmas Eve for the arrival of the “big guns”: two days of conditioning chemotherapy, headlined by a derivative of mustard gas. Its name is cyclophosphamide, and it works by sabotaging the machinery that copies DNA in rapidly dividing cells. As it does this, it breaks down to form toxic chemicals, including a pungent one called acrolein, which can destroy the lining of the bladder.
To neutralize its effects, patients must take another drug, called mesna, and drink plenty of water.
After a day of rest, Chris began a radiation therapy regimen so intense that it would have killed him if delivered in a single dose. Instead, his radiologists used a particle accelerator to fire X-rays at him in multiple bursts during morning and evening sessions over four days.
“You basically get into a tanning booth made out of clear Plexiglas,” he said.
Wearing nothing but a paper gown, Chris had to stay completely still behind two metal shielding blocks, each the size of a brick, positioned to protect his lungs from irreversible radiation-induced scarring. He did get a mild tan, he says, along with damaged skin that still resembles crepe paper.
Another absurdity still makes him laugh: while he requested punk rock for one of the sessions, he was instead blasted with the tune of Prince’s ‘Erotic City’.
When he finished the final round of total body irradiation on 30 December, the radiology team gathered for a final tribute and let Chris hit a small ceremonial gong.
Help from newborns
The morning of New Year’s Eve, Chris wrote on Facebook, “I’m as nervous as an expectant father!” An hour and a half later, he marked the delivery of his “zero birthday” with a small chocolate cake and a decorative “0” candle: the day when his own bone marrow cells, erased by radiation and chemotherapy, were replaced by roughly four tablespoons of a life-granting elixir from the cord blood of two baby girls.

Even with some of the best help that medicine can offer, transplant recipients face a daunting few weeks without functional bone marrow when nearly anything can kill them.
Chris and Bill have nicknamed the donors Amelia and Olivia based on their blood types, A-negative and O-positive. In a later post, Chris marveled at the new arrivals reseeding his bone marrow: “I use more vanilla flavoring creamer in my coffee than the volume of cells that are rebuilding my entire blood and immune system.”
Four hours after the initial infusions, he received his protective bridge of blood-forming stem cells, collected and expanded from the cord blood of a third baby, a boy he and Bill have nicknamed Eddie.
Less than three weeks after the transplant, Chris’s neutrophils had fully engrafted and genetic tests suggested that Amelia had decisively won the fight to form his new blood and bone marrow. He progressed so rapidly, in fact, that he had to stay in the hospital for two days after he was fit to leave, so that Bill could finish preparing the apartment.
28 January: discharge day. As his family packed up his hospital room, Chris was taking a shower when a wall of exhaustion hit him. He could no longer stand or even dry himself off and sat dripping on the shower bench until Bill heard his calls for help.
He had survived, but life had fundamentally changed.
At home, every surface had to be disinfected daily with a bleach solution. At first, Chris couldn’t walk 100 feet down the apartment hallway without leaning on his brother. Until he hit the 100-day milestone after his transplant, the end of the most vulnerable period for recipients, he returned to the Seattle Cancer Care Alliance every other day for blood tests and checkups.
On the 97th day, Chris and his family celebrated a hard-fought victory when he was officially declared cancer-free: a leukemia survivor.
Cord blood today
Despite dozens of studies documenting its curative powers, cord blood is saved after only 5 per cent of all US births. The rest is simply thrown away.
Michael Boo, chief strategy officer for the National Marrow Donor Program, estimates that only one in ten of those retained units passes the required screening tests and has enough volume to merit long-term storage.
Cord blood is also notoriously expensive, ranging from $22,000 to $45,000 per unit. Due to the relatively low demand from doctors, Boo says, public banks – at least in the US – are collecting as much as they can afford to keep. Beyond persuading new parents to donate, then, lowering the cost of cord blood transplants may depend upon persuading more doctors to use the cells and more insurers to cover them.
One potential use has attracted the avid interest of the Biomedical Advanced Research and Development Authority, part of the US Department of Health and Human Services. As part of Project BioShield, the federal agency has been on the lookout for medical interventions that could treat acute radiation syndrome after a dirty bomb or nuclear disaster.
Keeping people alive
Cord blood transplants in adults, still an option of last resort in the early 2000s, nearly slammed to a halt over the quandary of how to keep patients alive until their new bone marrow cells could kick in.
Some researchers reasoned that they could boost the transplant volume by giving adults two cord blood units instead of one. John Wagner and colleagues at the University of Minnesota performed the first double transplant in 2000, using cells from two infant donors.
The tactic dramatically reduced the rate of graft failure, in which the recipient’s body rejects the new cells. But it barely changed the time needed to regenerate the bone marrow, and some critics have questioned whether a double cord blood transplant offers any significant benefits.
Wagner says his research suggested that transplanting enough blood-forming cells was necessary ? but likely not sufficient ? for better results. Improved patient survival, in fact, seemed to depend more upon a revised roster of drugs given pre-transplant.

To their surprise, researchers also discovered that the donors in a double cord blood transplant seem to battle for dominance, a curious “graft-versus-graft” phenomenon that almost always results in the victor dominating the recipient’s new bone marrow and blood cells.
Filippo Milano, associate director of the Cord Blood Program at the Fred Hutchinson Cancer Research Center in Seattle, compares it to a pivotal scene in the 1986 movie Highlander, when the antagonist exclaims, “There can be only one!”

On a sunny morning nearly a year after Chris’s transplant, he and I meet the Italian-born doctor in his lab so he can greet one of his star patients and explain the science behind the therapy that saved Chris’s life. Milano is passionate about coaching soccer and cooking. On the side, he jokes, he conducts research on cord blood transplants.
Upon his arrival to “The Hutch” in 2009, Milano teamed up with Colleen Delaney, founder and director of the Cord Blood Program, to test and refine a treatment strategy that may yet prove a better option than a bone marrow transplant for people with leukemia who are at high risk of relapsing.
Based on collaborations and discussions with other experts in the field, Delaney pioneered a method to minimize the risk of infection and bleeding after a cord blood transplant by reducing the time needed for the new blood cells to kick in. The strategy relies on what she and Milano call an “expanded” blood unit.
Starting with an extra batch of cord blood, they separate out the minuscule fraction of blood-forming stem cells and their early descendants and expand that population in the lab.
The hundreds of millions – even billions – of resulting stem and progenitor cells can jump start the generation of protective blood cells in the recipient. When infused along with a more traditional transplant, they can act like a temporary bridge until the replacement bone marrow takes over. “The net gain was that you didn’t have those very prolonged periods of recovery,” Wagner said.

One crucial component, Delaney discovered, is a protein called Notch ligand.
When added to the blood-forming stem cells, Notch ligand lets them divide quickly in the lab but temporarily pauses their development by preventing them from maturing into the normal range of cell types. Critically, they never give rise to T or B immune cells, which would seek out and destroy any perceived threats lacking the proper “self” ID tags.
Join the conversation
Putting a donor’s T cells into an unmatched recipient, Delaney says, would trigger fatal graft-versus-host disease. “That’s the key: we get rid of all those bad parts of the immune system that need to be matched or they can kill you.”
The “bridge of recovery” lasts only so long before the full contingents of other donor cells begin attacking and dismantling it. But, with no cells checking IDs initially, the early flood of blood-forming stem cells need not be matched to the recipient at all, meaning that the “expanded” cord blood unit could be created well ahead of time and used whenever needed as a universal donor.
Other researchers are working on strategies toward the same end, and Mary Laughlin describes the overall progress as “very exciting”.
Delaney’s work, she says, “is very important, saving lives and improving the tolerability of these transplants and the success of these transplants”.

This is an edited extract from an article first published by Wellcome on Mosaic. It is republished here under a Creative Commons license.
Copyright 2015 The Wellcome Trust. Some rights reserved.